

What is Obstructive Sleep Apnoea (OSA)?
OSA is a disorder in which your airways repeatedly block during sleep. Each time this happens your brain wakes you up to make you start breathing again, resulting in fragmented, poor quality sleep. It usually occurs in people who are overweight and is due to a combination of increased tissue in the neck and relaxation of the neck and throat muscles during sleep. During the day it doesn’t occur as the neck and throat muscles keep the airways open.

Numbers vary from study to study but in some populations about a quarter of people are thought to have sleep apnoea. This percentage increases further in people with type 2 diabetes and obesity.
What are the symptoms?
You may be aware of unrefreshing sleep and daytime tiredness. You may be aware of repeatedly waking up and of feeling breathless when you do. If you have a partner they may have noticed both snoring and pauses in your breathing.

Who is at risk?
Being overweight or obese puts you at risk, as does having a large collar size, being male and being older. Alcohol and sedative medications are likely to make sleep apnoea worse. Other abnormalities of the airways eg. a small jaw or a large tonsils may be implicated.
If I think I might have OSA what should I do?
In the first instance you should make arrangements to see your family doctor for an assessment. If they agree that it sounds like OSA you are likely to be referred to a respiratory clinic for further assessment and potentially sleep studies.
As a first line assessment you may be asked to complete the “Epworth Sleepiness Scale” questionnaire. This is a questionnaire composed by Dr Johns in 1990. You rank yourself with the most appropriate number from 0-3 for each of eight different situations, then add up the total. The maximum score you can get is 24:
- 0 – would never doze
- 1 – slight chance of dozing
- 2 – moderate chance of dozing
- 3 – high chance of dozing
Situations:
- Sitting and reading (0-3)
- Watching TV (0-3)
- Sitting, inactive in a public place, eg. theatre or a meeting (0-3)
- As a passenger in a car for an hour without a break (0-3)
- Lying down to rest in the afternoon when circumstances permit (0-3)
- Sitting and talking to someone (0-3)
- Sitting quietly after a lunch without alcohol (0-3)
- In a car, stopped for a few minutes in traffic (0-3)
Results:
- 0-5 – Lower Normal Daytime Sleepiness
- 6-10 – Higher Normal Daytime Sleepiness
- 11-12 – Mild Excessive Daytime Sleepiness
- 13-15 – Moderate Excessive Daytime Sleepiness
- 16-24 – Severe Excessive Daytime Sleepiness
If your initial assessment is suggestive of OSA, sleep studies will be arranged. Some clinics will arrange for you to have a basic assessment at home. They will give you equipment to record your breathing movements and oxygen levels.
Alternatively, or following on from that you may be asked to attend a sleep centre for assessment. In this situation more a more detailed assessment can be carried out while you sleep.
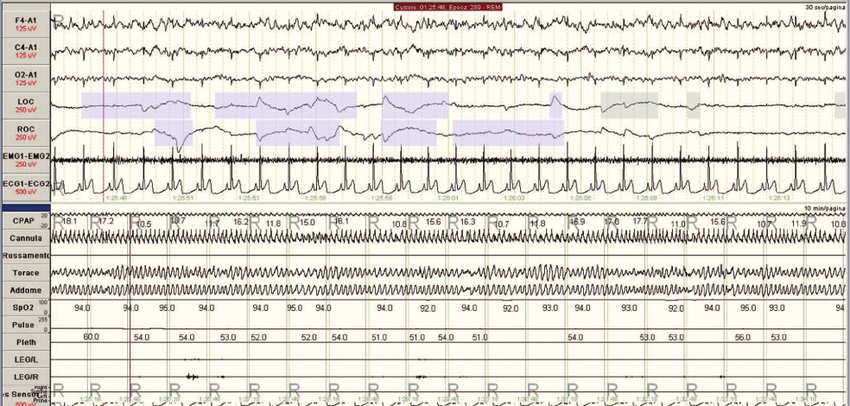
The severity of OSA is defined by the number of times breathing stops altogether (apnoeic episodes) and the number of times breathing is shallower or slower than normal (hypopnoeic episodes).
If I am diagnosed with OSA what treatments are available?
Treatments for OHA include lifestyle changes like losing weight, sleeping on your side or cutting down on alcohol.
For people with moderate or severe sleep apnoea a device called a CPAP machine can also be used (continuous positive airway pressure). This is a machine that is attached to a face or nasal mask. It provides a constant flow of air into the airways that keeps the airways open, avoiding episodes of apnoea. Fitting the mask properly can initially be awkward, and it can be uncomfortable if not done properly. This is usually a minor issue however and most people get used to it over a period of a few weeks and very pleased with the improvement in their sleep quality and the reduction in their drowsiness.

Information is still limited but in studies of people with OSA who also have type 2 diabetes, treatment with CPAP has been found to improve diabetes control. This seems to be particularly in those with more severe sleep apnoea and whose diabetes control was worse to begin with. In addition to potential improvements in diabetes control people who have been treated for OSA have a large reduction in their risk of stroke and heart disease, their life expectancy is also increased.
Finally, in rare situations, if people have a structural abnormality of their jaw or throat surgery may be a treatment option.
So, if you do have symptoms that may be in keeping with OSA, it’s definitely worth making an appointment with your GP to see if the feel further investigation is warranted.
References:
Effects of CPAP treatment on glucose metabolism in patient with OSA, Martinez-Ceron et al, – Sleep Medicine Reviews, Feb 2016
Obstructive Sleep Apnoea (OSA), British Lung Foundation, 2015